
The aim of this article is to provide advice and self help for people with tennis elbow or golfers elbow. The information is also presented in video format below.
The article is written on the assumption that the reader has been diagnosed with tennis or golfers elbow by a healthcare professional. If you haven't been diagnosed but you think you might have the condition then its best to get checked out first as there are other conditions that can cause similar symptoms.
1 - What is Tennis and Golfers elbow ?
 Well the first thing to say is that you certainly don't have to be a tennis player or a golfer to have tennis or golfers elbow, in fact it’s much more common in people who have never even picked up a tennis racket or swung a 7 iron.
Well the first thing to say is that you certainly don't have to be a tennis player or a golfer to have tennis or golfers elbow, in fact it’s much more common in people who have never even picked up a tennis racket or swung a 7 iron.
The names were first used in the late 1800's when it was noticed that elbow pain was commonly seen in people who played recreational tennis and golf at around that time. Mainly because the early rackets and clubs they were using were heavy and poorly designed compared to today’s modern equipment.
That’s not to say that golfers and tennis players of today don't get the condition, they certainly can do, but as we will learn, there is more to tennis and golfers elbow than just a simple sports injury.
 |
| Site of Pain in Tennis Elbow |
In tennis elbow it's the forearm muscles that cause wrist extension which come together to form a shared tendon called the common extensor origin. This attaches to the outside of the elbow at a bony area called the lateral epicondyle. And if you make a strong fist, you can feel the tendon tightening right at this point.

This is usually the area of maximum tenderness if you have tennis elbow. And you will already know this because you will no doubt bang the area numerous times a day, resulting in an outburst of unsavoury language.
A few other simple tests for tennis elbow are pain on gripping, and pain on resisted wrist extension - you can do this by reaching out in front of you (painful arm) with palm downwards, and then trying to keep your wrist straight while pushing it down with your other hand. Doing the same movement but with just your middle finger might be particularly painful as it concentrates the force through one of the forearm muscles called the ECRB, which tends to form the main part of the tendon that's most affected.
 |
| The Resisted Wrist Extension & Resisted Middle Finger Tests |
 |
| Site of Pain in Golfers Elbow |
2) Why have I got it ?
Both tennis and golfers elbows are overuse conditions. In tennis elbow, it's an overuse of wrist extension which overloads of the common extensor origin tendon and causes disruption of the tendon fibres. This is the movement associated with the backhand stroke in tennis which is where it gets its name but in modern life its more commonly associated with work related repetitive wrist extension activities such as computer or mouse use, and particularly gripping activities.

This is because we must extend the wrist in order to achieve full power, so any repetitive gripping activity can cause tennis elbow and we see it a lot in factory workers, plumbers, carpenters, butchers, decorators, mechanics, hairdressers, florists, machine operators and people who work with vibrating tools.

Of course, it's also seen in sports, particularly rackets sports, throwing sports, rowing and we see it in musicians, particularly pianists. It also doesn't have to be low level repetitive over-use. You can also get it with single bout of heavy gripping activity which I can attest to personally as I had tennis elbow myself a few years ago after carrying a very heavy bag of fossils for my geologist sister for just 20 minutes.
Golfers elbow is similar but involves repetitive wrist flexion as seen in the right wrist of a right-handed golfer during the golf swing. As with tennis elbow, it’s also common in throwing and racket sports, including tennis funnily enough, but it's the forehand action that stresses the common flexor tendon rather than the backhand as we see in tennis elbow.

In the workplace, golfers elbow is seen in similar occupations to tennis elbow but if I was to invent an activity that would be highly likely to cause golfers elbow, I would have someone repetitively turning a heavy revolving door or spinning a roundabout in a children's playground. It's that open handed slapping type movement that stresses the tendon and causes the condition.
So, to summarise, both tennis and golfers elbow are caused by overuse of the tendons involved in wrist movement, beyond a level that they can cope with, which then causes degenerative changes within the collagen fibres that make up the tendon. It can be single heavy use activity that you've done, like in my case of carrying the very heavy bag, or more commonly it’s a low-level repetitive overuse, sometimes over many months until the tendon starts becoming painful. It's also worth noting that you can have both tennis and golfers elbow at the same time in the same elbow.
Both conditions affect men and women equally with the most common age range between 35 and 55 years. Tennis elbow is by far the more common condition though, being about around 7 times as common as golfers elbow.
3) What can I do about it ?
Well, this is a good news and bad news situation. The good news is that 80-90% of people with tennis or golfers elbow with get better over time often without any treatment at all. The bad news is that it's a slow recovery. Symptoms can take an average of 1-2 years to settle down and even longer in those cases where the person doesn't or can't rest from the aggravating activity that is causing it. That's not to say that the pain will remain unchanged over 1-2 years and then suddenly get better. It doesn't tend to behave that way. Instead, It will usually hit a peak early on, then plateau, and then slowly improve. In my case, it took about 18 months to settle down completely without any treatment, and over the last 6 months it was just mild and niggly - and that's a fairly textbook recovery.
So, if you're happy to ride the tide and wait for a natural recovery then you might not need any treatment at all. You just need to be patient. However, if you are going to do this and let it get better by itself then it is important that you identify the activity that caused the condition and then stop doing it, or at least significantly reduce it.
If it’s a single event like in my case of carrying the heavy bag, then it's fairly easy to just not do that thing again, but for those of you who have a job that is the cause then it might prove to be more difficult. But you must reduce the stress through the tendon or you're going to prolong your recovery, or it might worsen until you are forced to rest it. Your work situation is going to be unique to you so if can't work out a solution yourself then talk to your employer or get an occupational assessment. It may be something as simple as using an ergonomic mouse and keyboard to neutralise your wrist position, or using a tool designed to reduce grip pressure.
 |
If it's a sports related problem then it might be best if you see a physio, a sports therapist or a coach familiar with managing these conditions. Things like technique, practice routine, racket string tension, grip width etc. can all contribute to this problem. So, unless it's something obvious, get checked out in order to address your specific issues.
 |
| Epicondylar Clasp - Amazon Link |
They work by absorbing some of the force when the forearm muscles pull on the tendon. As a quick experiment, to see if it will work for you, make a fist and then grip tightly until the pain starts. Then do it again but this time, with your other hand squeeze around the thickest part of your upper arm. In most cases you should feel that you can grip harder, with less pain while squeezing your forearm.
 |
| Compression Sleeve - Amazon Link |
Taping works in a similar way but it can be messy, difficult to apply yourself, be uncomfortable if you have hairy arms, and you need to reapply it regularly as it tends to lose its tension after a few hours. As such I don't tend to advise tape. The clasps, and compression sleeves are a much better option in my opinion.
Ok, so that might be enough for you, and indeed that's what I did with my tennis elbow. I just avoided painful movements, wore the clasp on bad days, but otherwise continued to use my arm normally, and it slowly got better over 18 months. The rest of this article will go on to explore the treatment options, so if you're happy with what you know now, your symptoms are manageable, and you want to just let nature takes its course, then you can stop reading. For the rest of you, let’s go on and take an honest look at the evidence for the treatment of tennis and golfers elbow.
Treatment Options
Now unfortunately, when you look at all the research, there really is no single reliable treatment for tennis or golfers elbow. There are things you can try that might work in your case, or they might not. You can get a feel of this uncertainly by simply googling tennis elbow or golfers elbow treatment and seeing the myriad of different suggestions that come up. And this should ring alarm bells that a simple cure just doesn't exist. So ignore anything you read about miraculous treatments claiming to cure the problem in a few days or weeks. If it gets better that quickly, it probably wasn't tennis or golfers elbow in the first place. It was probably just a simple muscle or ligament sprain.
Unfortunately, most of the treatments that you might come accross on the internet are not supported by the research. That includes things like therapeutic ultrasound, TENS, laser treatment, homeopathy, massage guns, deep friction massage or indeed any other hands-on therapy. A few days pain relief is about all you are likely to get with these treatments and that's not good value for something that could take 18 months to resolve. That’s not say they might not work for you, it’s just that the research doesn't support their use.
If you think about it though, assuming your tennis or golfers elbow is like mine was and is going to take 18 months to settle, and you decide to splash out and work your way through all the self-treatments suggested on the internet, then whichever of these treatments you are using at the 18 month point will be what you perceive as being the cure. You might then tell other people that this treatment worked for you. And that's how a lot of these so-called treatments gain traction, by word of mouth and not evidence-based research. Food for thought.
Treatments supported by Research
The treatments worth trying will depend on the severity of your symptoms. If your pain is severe, then you're certainly going to need to rest your elbow. The use of heat or ice can help with resting pain. Use a hot pack or a cold pack for 20 minutes at a time. Try both and see what works best for you.

At that point, you can either go with the flow and patiently wait for natural recovery as we've already discussed, or you could try to speed things up by using some of the treatment options that we will now discuss.
Of all the treatments available, exercises have the best overall evidence base. They do require a commitment in time and effort over many months, and in my experience, other than professional and keen amateur sports people, not many folk, myself included, have the patience and strong mindedness to do them regularly in the quantities needed.
The main rule with exercises is that they should be pain free. Therefore, they aren't a good idea if you have more severe pain as you won't be able to do them without aggravating the condition. So, the pain must have settled down to a mild or manageable level before you use them.
Exercises work by slowly increasing the strength and resilience of the tendon until it can cope better with the workload you are asking it to do. Changing a degenerative gristly tendon into a healthy lean tendon takes time, and we are talking about months rather than weeks. Those collagen fibres will respond to exercise and load but it's a slow process, and that's why patience and commitment are required.
I have written separate articles which describe a detailed exercise programme for both tennis and golfers elbow below.
 |
| Link to an Exercise Programme for Tennis Elbow |
 |
| Link to an Exercise Programme for Golfers Elbow |
_____________________________________________________________________________
For the other treatments we will discuss you will need to see a clinician.
These used to be a commonly performed procedure as they can undoubtedly provide some pain relief, but the effect usually wears off within a few weeks and then the patient comes back wanting another one, and then another one. And the most current research has found that patients who have repeated cortisone injections can develop a degree of structural weakness within the tendon which can actually prolong the condition and makes it more likely that they will have another episode in the future.
 |
| Tennis Elbow Cortisone Injection |
So basically, in the long-term cortisone can cause exactly the opposite effect of what you want to achieve as a clinician. The cortisone basically reduces the resilience of the tendon and makes it more vulnerable to injury in the future. As a result, I rarely offer cortisone injections now and if I do, its only in very specific cases and only ever as one off.
For more information about cortisone injections, click here.
___________________________________________________________
The other treatments I'm going to talk about all work on the premise that Tennis and Golfers elbow can be considered a type of injury where the tendon healing process becomes stuck and by trying to re-injure the affected tendon in a controlled way, we can try to kick start this healing process and stimulate recovery of the degenerative tendon fibres. These treatments are used on many different chronic tendon and soft tissue problems such as achilles tendonitis, plantar fasciitis and lateral hip pain as well as tennis and golfers elbow.
The first of these 'provocative treatments' is Extra Corporeal Shockwave Therapy (ECSWT). This is a treatment which uses high pressure sound waves to disrupt the collagen fibres in a way that stimulates a healing response. It's a treatment that usually lasts around 10 minutes and is typically delivered once a week over a 3-week period.

Shockwave treatment can cause a temporary increase in pain as it is essentially re-injuring the tendon in a controlled way in order to prod it into kick starting the healing process. The evidence for ECSWT is fairly mixed, with some studies finding it can be helpful in reducing pain and increasing during the early stages of the condition.
Dry Needling / Needle Fenestration
Another way of trying to stimulate this healing response is to cause some bleeding around the tendon. We know that blood contains various growth and repair factors that initiate healing when you have an injury. By high jacking this system we can try to encourage the tendon to repair itself. The easiest way of doing this is by using a needle to cause some disruption and local bleeding. Acupuncturists can do this, but it can an uncomfortable process. A better way is using some local anaesthetic and then inserting a normal injection needle under ultrasound image guidance directly into the painful part of the tendon.
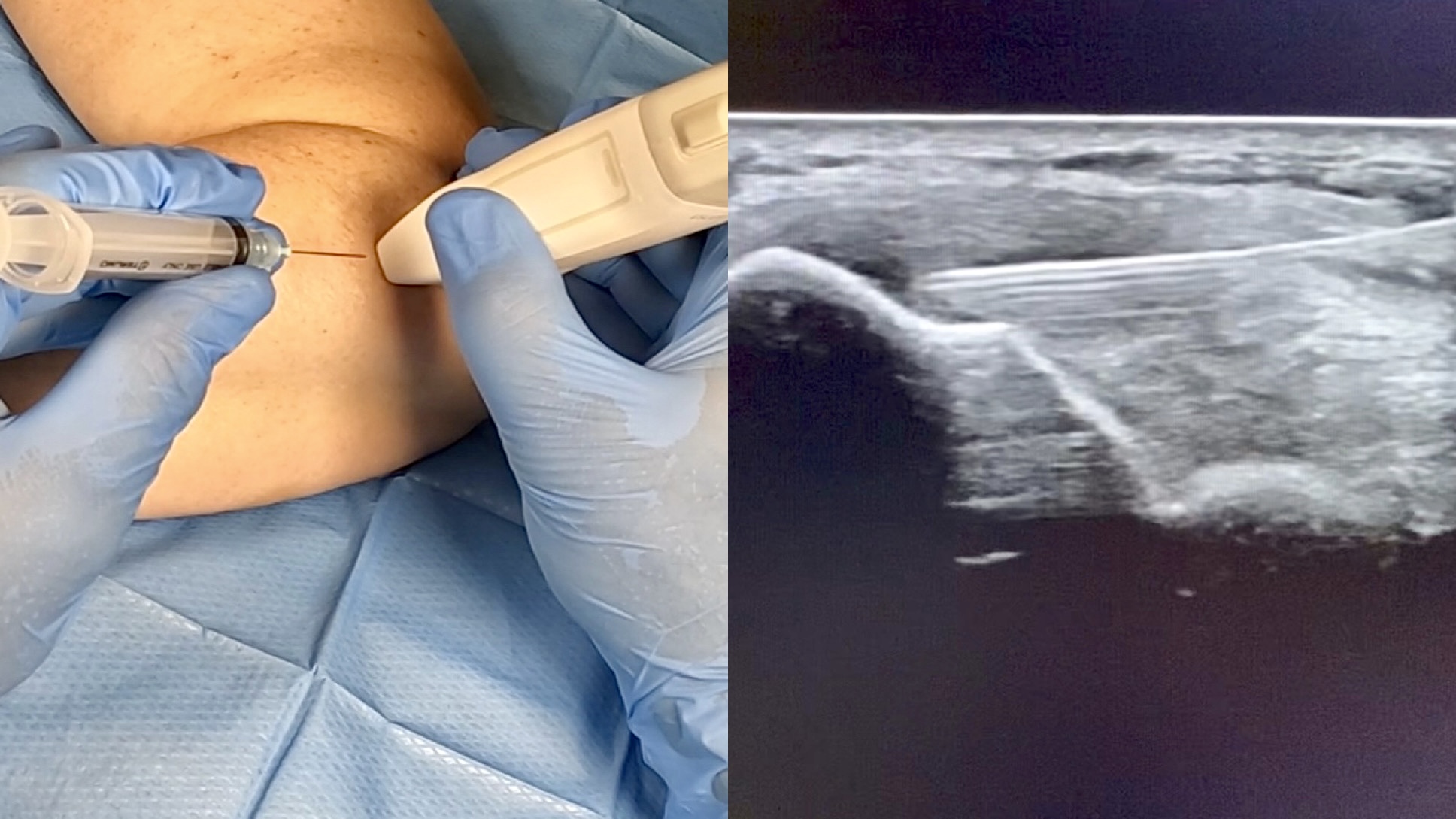 |
| Needle Fenestration of the common extensor origin in Tennis Elbow |
The needle tip is then used like a mini scalpel in order to 'injure' the collagen fibres. Because you are trying to cause local inflammation, you should not use anti-inflammatory medication like ibuprofen for 2 weeks before or after the procedure. This is called 'dry-needling' or 'needle fenestration' and it is considered a healthier alternative to a cortisone injection.
Platelet Rich Plasma (PRP) Injection
The latest treatment technique takes this process a step further. A process called PRP, involves taking some blood from the patient, spinning it in a centrifuge and then separating out the platelets which contain all those growth and repair factors, and then injecting this concentrated ‘Platelet Rich Plasma’ back into the tendon. PRP is becoming more widely available, but you might struggle to find it being offered on the NHS at the moment because it’s an active area of current research and the jury is still out regarding its overall effectiveness.
Surgery
And finally, for the most severe cases that have resisted treatment and the passage of a few years, surgery might be considered. This is usually a last resort option as it doesn't work for everyone. Less than 5% of all cases get to the stage of surgery but if you've had intrusive symptoms for a few years then it might be worth seeing an elbow surgeon.
This article provides general information related to various medical conditions and their treatment. It is intended for informational purposes only and not a substitute for professional advice, diagnosis or treatment provided by a doctor or other qualified health care professional. The information provided does not constitute personal advice or guarantee of outcome and should not be used to diagnose yourself or others. You should never ignore advice provided by a health care professional because of something you have seen or read on this website. You should always consult a doctor or other qualified health care professional for personal medical advice.